Sample Undergraduate 2:1 Environmental Sciences Dissertation
See for yourself why we're a leading academic writing company. One of our expert writers has created this bespoke sample Environmental Sciences dissertation that shows the quality of writing that's guaranteed with every piece of work ordered. Secure your academic success and place an order today or view our Dissertation Writing Service.
Factors Influencing Sanitation Conditions in Ghana
Abstract
Sanitation and hygiene practices can have a significant impact on the health of individuals and constitute a substantial factor in the transmission of diseases. In developing countries, the provision of adequate sanitation services is an issue which has not been thoroughly addressed. The aim of the research study was to assess the use of sanitation services and hygiene practices in Ghana and to identify factors, particularly socio-cultural factors, which may influence the use of these services. A systematic literature review was conducted to identify relevant research studies published in 2012 or later. The majority of identified relevant publications were found to have occurred in low-income populations. It was found that there are very few private sanitation services: the majority of the population either use public sanitation services, defecate in the home environment or practise open defecation. A substantial portion of the respondents indicated that they did not use the public sanitation services due to cost, poor management, safety fears or lack of privacy. The defecation practices which are engaged in by the majority of low-income populations in Ghana are likely to contribute significantly towards the transmission of diarrheal diseases and are a contributing factor to high child mortality rates that urgently need to be addressed.
Chapter 1 – Introduction
1.1 Introduction
Water is a highly effective disease vector (Hunter, 2003). A contaminated water resource can rapidly affect the utilising population, spreading diseases that can result in severe and prolonged health impacts and even death (Pruss et al., 2002). However, water is a necessity of life and some populations have no alternative options to using contaminated and unsafe water resources (Wright et al., 2016). At the current time, it is estimated that approximately 2.1 billion individuals across the world do not have access to safely managed drinking water resources (WHO/UNICEF, 2017). Whilst the use of unsafe water is the vector by which diseases can be spread, the processes that result in unsafe water resources must also be considered as an intrinsic aspect of the issue. Thus, sanitation and hygiene practices are integral to the ideal of safe water provision for all.
In 2016, the United Nations (UN) issued their Sustainable Development Goals, comprised of 17 key goals for aiding sustainable development (UN, 2018). Goal 6 is ‘ensure access to water and sanitation for all’ (UN, 2018). Goal 6 encapsulates the fact that clean water, sanitation and hygiene are intrinsically linked and that high standards in all three aspects are necessary to prevent the spread of disease and to ensure good health and well-being (goal 3 of the UN Sustainable Development Goals; UN, 2018). It has been estimated that approximately 80% of the wastewater produced globally is not treated before discharging into the natural environment (UNESCO, 2017). This factor is a highly likely contributor to the contamination of water resources with fecal matter. It is thought that approximately 1.8 billion individuals are utilising water resources that are contaminated by fecal matter (UN, 2016). A lack of access to clean water and appropriate sanitation services is predominantly an issue in developing countries, in particular those in Africa (see figure 1; Pruss-Ustun et al., 2014). Prior to the UN Sustainable Development Goals, the Millennium Development Goals were implemented by the UN. Under the Millennium Development Goals access to clean water has increased substantially: it has been reported that over 90% of the global population has access to clean water (WHO, 2018). However, sanitation services have not experienced the same level of improvement - it is estimated that only 68% of the global population has access to at least basic sanitation services (WHO, 2018). In figure 2, the use of at least basic sanitation services in each country is shown. It is evident that the provision of clean water resources and sanitation services is lacking in many African countries in comparison to the wider world. The lack of progress in improved sanitation services has been suggested as a factor which is threatening the status of the clean water progress (Monney and Antwi-Agyei, 2018).
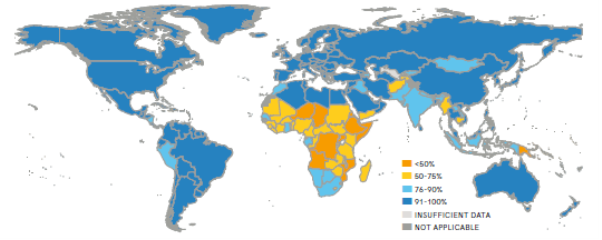
Figure 1. On a country basis, the proportion of the population utilising at least a basic drinking water service in 2015 (JMP, 2017 p.3).
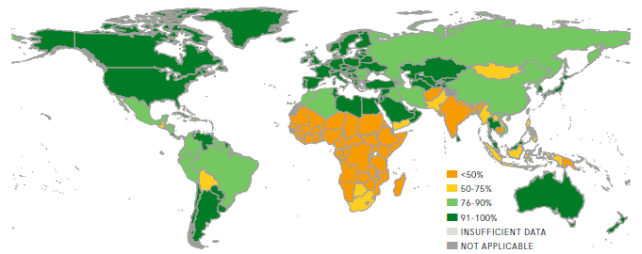
Figure 2. On a per country basis, the proportion of the population utilising at least a basic sanitation service in 2015 (JMP, 2017 p.4).
Hygiene practices are also a contributing factor to the global issue. Whilst data is more limited regarding global hygiene practices, in figure 3 limited data is shown detailing the availability of basic handwashing facilities. As with clean water and sanitation services, the provision of handwashing services in Africa is lacking.
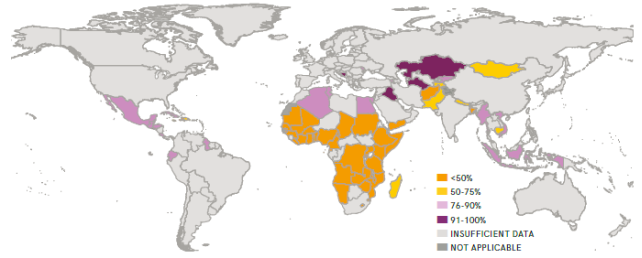
Figure 3. On a per country basis, the proportion of the population with at least basic handwashing facilities including soap and water at home in 2015 (JMP, 2017 p.5).
In general, Sub-Saharan Africa has experienced lower rates of improvement in sanitation and hygiene than other locations (Fuller et al., 2016). The rates of improvement also vary substantially between countries of Sub-Saharan Africa (Munamati et al., 2016). Ghana is an example of a country that has achieved significant progress in access to clean water. Under the UN Millennium Development Goals, Ghana achieved the target for clean water provision ahead of the 2015 deadline (Monney and Antwi-Agyei, 2018). However, the progress in sanitation services and hygiene practices has not been as rapid and has been suggested to be a factor which may threaten the progress made in clean water provision (Monney and Antwi-Agyei, 2018). Sanitation and hygiene development strategies were implemented in Ghana alongside water improvement programmes yet have not seen the same success. For example, in 2012 13.7% of the Ghanaian population had access to safe toilets; by 2015 this figure had only marginally increased to 14.3% (Centre for Science and Environment, 2018). The lack of success of improvement programmes suggests that there are underlying influencing factors which need to be understood to enable the development of targeted strategies to overcome these barriers, thereby preventing a lack of sanitation services and poor hygiene practices from undoing the progress made in clean water services.
If you need assistance with writing your dissertation, our professional Dissertation Writing Service is here to help!
Find out more1.2 Aim and Objectives
The overall aim of this research study is to assess the factors that have influenced sanitation services and hygiene practices in Ghana. This aim was developed from the clear gap identified between the progress made in improvements to clean water access and improvements to sanitation services and hygiene practices in Ghana even when all three have been prioritised. To achieve the aim of this research, the following objectives will be met:
- To review the current situation in Ghana including the currently and historically implemented improvement programmes.
- To identify links between sanitation services, hygiene practices and diseases/deaths in Ghana.
- To assess what factors are influencing sanitation services and hygiene practices in Ghana and how these factors are exerting influence.
- To develop recommendations for further action strategies to improve sanitation services and hygiene practices in Ghana and the wider world.
The attainment of these objectives will allow robust and accurate conclusions to be drawn related to the overall research aim, which will enable recommendations to be developed for further policy and improvement action strategies for both Ghana and the wider world.
If you need assistance with writing your dissertation, our professional Dissertation Writing Service is here to help!
Find out moreChapter 2 – Literature Review
In the following chapter a review of the current literature is presented. The topics covered in the literature review include: how sanitation and hygiene practices can influence the spread of disease, what factors can potentially influence sanitation and hygiene practices, and the Ghanaian situation.
2.1 Sanitation, hygiene practices and disease
There are five categories which are commonly used to describe the status of sanitation services, from most desirable to least desirable. These categories are:
- Safely Managed
- Basic
- Limited
- Unimproved
- Open Defecation (JMP, 2017).
Safely managed sanitation services are those where individuals are able to excrete hygienically and the excreta is either contained and treated in-situ, or treated prior to final disposal ex-situ (Mara et al., 2010). Basic sanitation services are those which are classed as improved sanitation service that are not shared (JMP, 2017). Limited sanitation services are those which are shared between households (JMP, 2017). Examples of unimproved sanitation services include buckets and pit latrines with a hanging slab (JMP, 2017). Open defecation occurs when there are no available sanitation services.
In terms of potential impact on health, the least desirable sanitation categories are those which are most likely to have an adverse impact on human health. There are two key reasons for this potential health impact: firstly, the more basic the sanitation service then the lower the likelihood of there being facilities available for handwashing with soap subsequent to service use. Secondly, there is a higher potential of fecal contamination of water resources if the sanitation services do not provide for adequate treatment and disposal of excreta (Berendes et al., 2017). In figure 4 the pathways for feco-oral disease transmission are shown - it is evident that adequate sanitation and hygiene practices are vital to prevent the spread of disease through fecal matter.
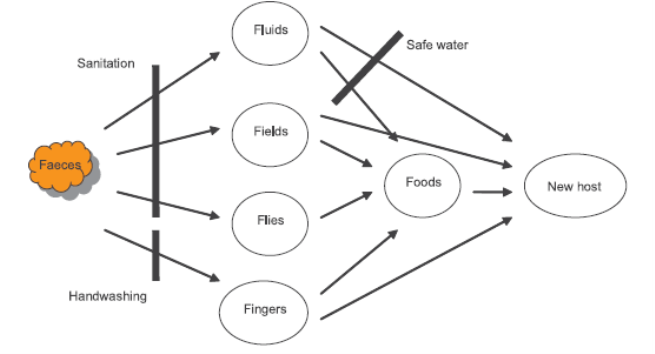
Figure 4. The faeco-oral disease transmission pathways and the points where appropriate sanitation service, hygiene practices and safe water can break the transmission pathways (Mara et al., 2010 p.2).
Fecal matter disease transmission is a significant factor in human diseases. In particular, diarrheal diseases are a significant concern. A study conducted by Eisenberg et al., (2007) found that even in scenarios where safe water is available, if the sanitation conditions are lacking then there is a minimal impact of water quality improvements in terms of reducing disease transmission. It has also been found that there are variations in the success of transmission reduction with the implementation of different sanitation improvements. Wolf et al., (2014) found that even in scenarios where the sanitation is described as improved, there is still relatively high potential for disease transmission.
If you need assistance with writing your dissertation, our professional Dissertation Writing Service is here to help!
Find out more2.1.1 Diarrheal disease burden due to poor sanitation and hygiene practices
The impact of diarrheal disease is disproportionate: children under the age of 5 are most likely to suffer adverse health impacts due to diarrheal diseases (Hetherington et al., 2017). It has been estimated that more than 800 children under 5 die from diseases, predominantly diarrheal, linked to unsafe water, inadequate sanitation and poor hygiene practices (Liu et al., 2016; UN, 2016). In figure 5 a comparison between a lack of access to improved water and sanitation service and deaths in children less than 1 year old is shown. It is evident that there is a higher rate of childhood mortality in regions with lower access to improved sanitation and water resources, which are predominantly classed as developing regions (Ashbolt, 2004). Baker et al., (2016) reported that limited sanitation services, even when shared between only 1 or 2 other households, were a factor increasing the risk of diarrheal diseases in young children. However, this was found to be impacted by the standard of the shared sanitation facility and whether there is access to adequate handwashing stations (Baker et al., 2016).
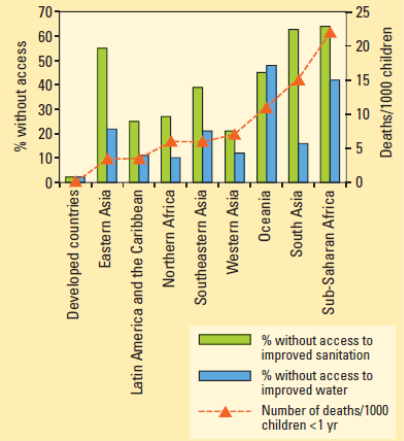
Figure 5. The percentage of populations without access to improved sanitation and improved water by region in comparison to the number of deaths per 1,000 in children less than 1 year old (Montgomery and Elimelech, 2007 p.18).
A meta-analysis conducted by Pruss-Ustun et al., (2014) which examined data collected from 145 countries suggests that in 2012 approximately 280,000 deaths could be attributed to inadequate sanitation and 297,000 deaths to inadequate hand hygiene. When all three aspects (safe water, sanitation and hygiene practices) were considered, it was found that 842,000 deaths in total were attributable to diarrheal diseases linked to these risk factors (Pruss-Ustun et al., 2014). In the same study, it was estimated that 361,000 deaths in children under 5 could have been prevented by access to improved water, sanitation and adequate hygiene practices (Pruss-Ustun et al., 2014). Similar studies have reported the link between all three aspects, with findings typically suggesting that synergistic improvements are needed addressing all three aspects to enable a significant reduction in the potential for diarrheal disease transmission, particularly in young children (Fuller et al., 2015; Lakshminarayanan and Jayalakshmy, 2015; Wolf et al., 2018).
2.2 Factors other than service provision influencing sanitation and hygiene practices
Arguably the most obvious factor influencing sanitation and hygiene is the provision of services and infrastructure - as previously mentioned, there are different categories of sanitation services that are globally recognised. Current evidence suggests that only safely managed sanitation and basic sanitation services will substantially contribute towards a reduction in the transmission of diarrheal diseases (Baker et al., 2016). However, it is not solely the provision of infrastructure for sanitation and hygiene practices that can potentially influence improvements in these factors.
From an economic perspective, it has been identified that there is a variation in the potential health risk to individuals due to economic status (Williams et al., 2016). Rheingans et al., (2012) found that there is a disproportionate occurrence of diarrheal disease in individuals classed as low-income: whilst this was predominantly due to the availability of sanitation services and the hygiene practices implemented, it was suggested that the lower nutritional status was an additional factor increasing susceptibility. Additionally, there was found to be a rural-urban divide, where the urban population was found to be more susceptible to diseases from inadequate sanitation and hygiene practices due to the higher population density, even when the rural populations were found to have lower-quality services (Rheingans et al., 2012). The higher population density is likely to be a contributing factor due to an increased number of individuals utilising the same services (especially in the case of shared sanitation services) and a greater ease of disease transmission between individuals due to increased contact. This would suggest that the provision of safely managed sanitation and infrastructure for best hygiene practices would provide a solution to disrupting the pathways for disease transmission. However, it has been highlighted in other studies that there are additional factors, aside from purely economical influences, that present barriers to improvements.
Pfadenhauer and Rehfuess (2015) conducted a study in the Philippines and found that there was a significant behavioural component which influenced the potential success of improved sanitation and hygiene practices. Habit was found to be a driving factor in the sanitation and hygiene practices used by participants in the Pfadenhauer and Rehfuess (2015) study, with children found to emulate the behaviours observed in their parents (Assefa and Kumie, 2014). Dreibelbis et al., (2015) also found that existing behaviour patterns had an influence of the use of sanitation services. In India, it was found that in a high number of cases individuals continued to practise open defecation even when a functioning latrine was available (Dreibelbis et al., 2015). It was suggested that this was primarily due to a combination of existing behaviour patterns and the influence of cultural beliefs/practices (Dreibelbis et al., 2015). This suggests that behavioural and cultural practices need to be addressed to increase the uptake in improved sanitation use and hygiene practices improvements. The influence of cultural practices is likely to vary between communities and different regions, due to differences in cultural practices. For example, among some communities it is prohibited for opposite genders to use the same toilet (Lawrence et al., 2016). This highlights the importance of understanding the cultural practices of the specific region of intervention to ensure that targeted action strategies can be developed.
O’Reilly and Louis (2014) suggest that there is a strong influence of social factors on the success rate of improved sanitation service use and good hygiene practices. It was found that in India, a combination of political support, social pressure and political ecology (for example access to water) were the major influencing factors for increased use of sanitation services and good hygiene practices (O’Reilly and Louis, 2014). Similar findings regarding the influence of social pressures have been reported in other published studies (Pfadenhauer and Rehfuess, 2015; Lawrence et al., 2016). This has often been found to occur as a result of an increased prevalence of education programmes explaining why improvements in sanitation and hygiene practices are necessary (Akter and Ali, 2014). It is evident that the prevalence of other factors influencing sanitation and hygiene practices are tied closely to specific region, especially in the case of social and/or cultural practices. This suggests that outside of service provision programmes it will be important to understand the existing socio-cultural factors to enable the development of targeted improvement programmes.
2.3 The Ghanaian Situation
Over 20% of the Ghanaian population use surface waters to meet their daily needs - this is nearly 6 million individuals (Water, 2018). Concurrently, approximately 67% of the population do not have access to improved sanitation, with many having no access to any sanitation services, approximately 18 million individuals (Water, 2018). Although Ghana met their target for improved water resources established under the UN Millennium Development Goals, improvements in sanitation have been substantially lower and the target for improvements was not reached (Alagidede and Alagidede, 2015). During the time period for the UN Millennium Development Goals, the access to basic sanitation services increased from 6 to 15% in 15 years, a very minimal rate of increase. The UN has reported that since 2011 the access to basic sanitation services has remained static at 15%, with a high rate of individuals continuing to practise open defecation (UN, 2018). The lack of progress in sanitation and hygiene practices has been acknowledged, and targeted improvements, including education programmes, have been outlined in the Ghanaian government’s National Community Water and Sanitation Strategy (NCWSS, 2014). Additionally, there is a substantial difference between the access to sanitation services in rural communities in comparison to urban communities. Akpakli et al., (2018) reported that 19% of urban populations have sanitation services access, whereas only 8% of rural populations have the same access.
There have been reported decreases in the rate of child mortality (in children under 5 years of age; Arku et al., 2016). Arku et al., (2016) investigated the child mortality rates in Ghana between 2000 and 2010 and found that there was a decrease in mortality rates across all districts (see figure 6). It is likely that the access to improved drinking water and improved sanitation services over this time period contributed to the decrease in the child mortality rate (see figure 7; Arku et al., 2016).
The burden of diarrheal diseases in children under 5 in Ghana remains relatively high. A study conducted by Kumi-Kyereme and Amo-Adjei (2016) examined the incidence of diarrhoea in Ghanaian children in relation to the socioeconomic characteristics. It was found that there was no difference in the diarrhoea rates of children in households with improved drinking water resources compared to those with unimproved (Kumi-Kyereme and Amo-Adjei, 2016). However, it was found that there was a significant difference in the reported diarrhoea rates of households with unimproved sanitation facilities, which were found to have a higher reporting of instances of diarrhoea, in comparison to households with improved sanitation facilities where lower rate of diarrhoea were reported (Kumi-Kyereme and Amo-Adjei, 2016). Wang et al., (2017) investigated the exposure of children in 4 neighbourhoods of Accra in Ghana to fecal contamination. It was found that there was a lower exposure rate among children in higher-income areas with access to more improved sanitation services (Wang et al., 2017). In comparison children in lower-income neighbourhoods with lower access to sanitation services and higher rates of open defecation were found to have significantly greater rates of exposure to fecal contamination (Wang et al., 2017).
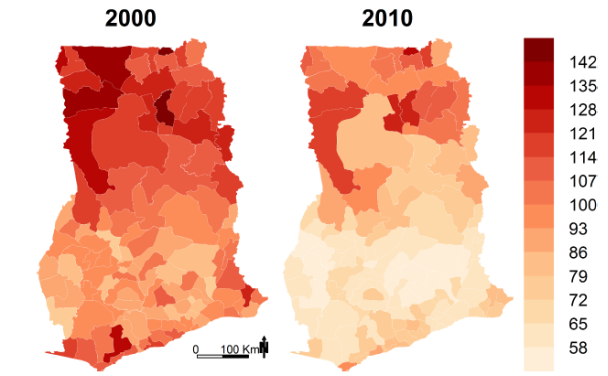
Figure 6. Mortality rates for children under 5 in deaths per 1,000 live births on a per district basis for 2000 and 2010 (Arku et al., 2016 p.7).
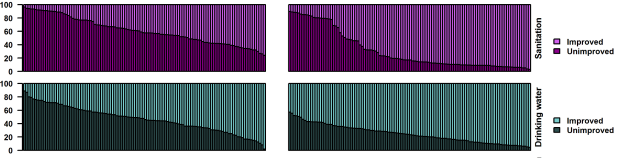
Figure 7. The access to improved/unimproved drinking water and sanitation service in Ghana for 2000 and 2010. Each bar represents one district (Arku et al., 2016 p.8).
It has been suggested that whilst there has been a decrease in the rate of child mortality in Ghana, recently the rate of decrease has stalled and no significant decrease in child mortality rate has been achieved over the past few years (Acheampong and Avorgbedor, 2017). One potential explanation for this is the continued high rates of diarrheal diseases among young children in Ghana. Research has indicated that the high level of access to improved water resources means that these continued high rates are unlikely to be primarily due to contaminated water resources (Kumi-Kyereme and Amo-Adjei, 2016). A lack of access to sanitation services and poor hygiene practices have been suggested as potential explanations for the persistence of relatively high child mortality and diarrheal disease rates (Ritter et al., 2018).
If you need assistance with writing your dissertation, our professional Dissertation Writing Service is here to help!
Find out more2.4 Summary
In summary, it is evident that whilst substantial progress has been made in the provision of safe water resources to the Ghanaian population, this has not been matched by improvements in access to adequate sanitation services or with improvements in hygiene practices. Although sanitation and hygiene have been focal points of government policy and action strategies, including non-governmental organisation-led programmes, there has been a very low relative rate of access improvement. It is a cause for concern as the poor sanitation services access and poor hygiene practices may counter the improvements and progress made in clean water provision. It is suggested that inadequate sanitation and hygiene practices are also a contributing factor to the stalling of the decrease in childhood mortality rates which has been identified subsequent to 2015. It is therefore important that the factors which are impacting the low rate of sanitation services growth and the poor hygiene practices are understood so that targeted action strategies can be developed.
Chapter 3 – Methodology
3.1 Research Design
It is the philosophy that is applied which will shape the design of a research study. In scientific research there are two major philosophies which are commonly applied: either the philosophy of positivism or the philosophy of interpretivism. Under the theory of positivism, the world is considered as objective and external to the researcher. This translates to the idea that it possible to quantify all aspects of the world by measurement and assignment of a numerical value without the act of measuring altering that which is measured. The resulting numerical values can then be analysed statistically using established statistical procedures stemming from scientific principles (Sobh and Perry, 2006). This results in findings which are quantitative. There is no consideration for how human perceptions, opinions or interests could potentially influence the research or data which is collected. Whilst this holds true for many aspects of scientific research, there is a growing body of literature which suggests that taking a positivist-based approach is not suitable for the characterisation of real world scenarios due to the lack of allowance for human influence, such as opinions. This issue is typically encountered when there is a social aspect to the proposed research. In this instance the theory of interpretivism may be a more applicable philosophy to guide the research design.
The theory of interpretivism suggests that there is need for a greater variety of data to be captured, rather than purely numerical values (Rolfe, 2006). In this manner it is possible to account for non-objective occurrences, such as the perception of an individual. Research studies shaped by interpretivist ideals will typically result in a dataset formed of qualitative data. In this instance it is typically not possible to use statistical methods to analyse the collected data and therefore the analysis will generally be presented in a narrative format (Feilzer, 2010).
3.2 Research Protocol
It was determined that a systematic literature review would be the most appropriate methodology to apply to this research study. The aim of a systematic literature review is to identify, critically evaluate and integrate the findings of all relevant studies (Cooper, 2003). Therefore, the data which was collected was secondary in nature. A systematic literature review was selected due to the nature of the research topic. The overall aim of the study was to develop a comprehensive understanding of the socio-cultural and demographic factors influencing sanitation conditions in Ghana - therefore, the use of existing research was determined as suitable. A systematic literature review was selected as the methodology due to the potential for this methodology to include all relevant currently published research. The inclusion of all relevant research improves the accuracy and reliability of the conclusions that were drawn due to enabling the critical comparison of multiple data resources, thus increasing the potential for the identification of outlying data points/sets. This will allow for the identification of relationships, contradictions, knowledge gaps and inconsistencies in the published literature (Khan et al., 2003).
3.2.1 Systematic literature review method
In the following sections each step that was followed in the process of conducting the systematic literature review is outlined.
3.2.1.1 Scoping
The research question which was developed and formed the scope of this study was: Why has there been a lack of progress in sanitation and hygiene improvements in Ghana? As a secondary research question, it was also asked: How are sanitation and hygiene practices in Ghana impacting the child mortality rate? These two questions were used as the basis for the development of the search terms used to identify the research studies potential relevant to the systematic literature review. The search terms selected were: ‘Ghana’, ‘sanitation’, ‘hygiene’ and ‘child mortality’. These search terms were combined with Boolean operators to perform keyword searches of the Google Scholar public database.
3.2.1.2 Inclusion and exclusion criteria
The identified research studies were processed through the pre-determined inclusion and exclusion criteria using the title and abstract of each study only as the primary screening step. The inclusion criteria which were applied were as follows:
- In English
- Published study
- Published 2012 or later
- Use data pertaining to 2008 or later
- Focused specifically on Ghana
- Include socio-cultural and/or demographic factors as the main foci of the study
- Analyse sanitation or hygiene practices
The exclusion criteria which were applied are as follows:
- In a language other than English
- Primary data from a period prior to 2008
- Publication date before 2012
- Unpublished study
- Primary focus was safe water
- Investigated a country other than Ghana
- The format of the study was a review
At the screening stage 5.865 studies were excluded due to either not meeting the inclusion criteria and/or meeting at least one of the exclusion criteria.
The next step which was taken was to determine the eligibility of the studies not excluded in the primary screening of the title and abstract. Each of the remaining studies was examined in detail to determine whether the study complied with the inclusion criteria and did not meet any of the exclusion criteria from details not included in the title or the abstract. At this stage a further 214 studies were excluded. There were found to be 11 studies remaining which were classified as meeting all the inclusion criteria and thus were deemed suitable for inclusion in this research study. The relevant data was extracted from each of the selected studies and entered into an Excel spreadsheet. The data which was extracted from each study included the following:
- Author/s
- Publication date
- Study location
- Study participates/demographic
- Time period of data collection
- Study methodology
- Aspect of study focus (sanitation services/hygiene practices/child mortality)
- Study findings
Due to the variation in the format of the identified studies (a combination of quantitative and qualitative data was identified as relevant) it was determined that a qualitative research synthesis based on a critical narrative analysis was the most appropriate analytical approach to adopt.
3.3 Ethical considerations
As this research study was conducted using secondary data, there were no direct ethical considerations which needed to be accounted for. All data which was used within the study needed to be attributed to the primary authors, and this was achieved through the use of an established referencing protocol, namely the Harvard referencing system.
Chapter 4 – Findings
The characteristics of the included studies are detailed in table 1. The studies conducted by Crocker et al., (2017) and Greenland et al., (2016) were both assessments of the impact of improvement programmes. All the other identified studies were condition assessment studies that focused on characterising the available sanitation facilities in the study areas and the use of these facilities by the inhabitants.
4.1 Sanitation Services and hygiene practices
The majority of identified studies that met the inclusion criteria were found to have been conducted in low-income urban areas. Only one study was identified that specifically examined hygiene practices in the form of the availability of handwashing facilities, where it was found that the possession of a private sanitation service was equated with a 25% greater chance of including handwashing provisions (Greenland et al., 2016). Fiasorgbor (2013) found that only 1 public sanitation service provided soap and towels to users - the reason given for this was that when these materials had been provided previously they were stolen, and therefore the majority of facilities ceased providing them.
In general, it was reported that there was a low frequency of private, within-home improved sanitation facilities. This was found to be true even in the two studies (Akapakli et al., 2018 and Fiasorgbor 2013) where some areas of relatively higher-income were investigated. All studies found that either there was a predominant reliance on public sanitation services, or open defecation was practised. Those that did not have improved sanitation services and chose not to use the public services or openly defecate were typically found to defecate in bags or containers in the household environment which were then disposed of either in the garbage or street drainage systems (Hurd et al., 2017). Where respondents were dependent on public unimproved sanitation services, a high level of dissatisfaction with the services was typically reported across all studies. Complaints commonly cited included: smell, lack of management/upkeep, high cost of use (pay per visit), unsafe conditions and difficulty in access.
In two studies it was found that participants were unwilling to state that they practised open defecation; however site observations by the researchers identified open defecation as a common practice (Adubofour et al., 2013; Monney et al., 2013). It was suggested by Adubofour et al., (2012) that the lack of willingness to confirm open defecation practices was due to a sense of shame and humiliation that the practice created in the participants.
Table 1. The characteristics of each study included in the systematic literature review.
|
Author/s |
Published Date |
Study Location |
Study Participants/ demographic |
Time Period of Data Collection |
Method |
Design |
Aspect of Focus |
|
Adubofour et al., |
2012 |
Kumasi |
Households primarily Muslim Low-income urban neighbourhoods |
2009 |
Survey |
Cross-sectional randomised |
Sanitation |
|
Mazeau et al., |
2012 |
Ashaiman - Southern |
Urban, planned (Nii), indigenous (Oko) and spontaneous (Amui) city areas |
Not stated |
Survey |
Cross-sectional survey |
Sanitation |
|
Monney et al., |
2013 |
Accra |
100 residents Low-income urban neighbourhoods |
Not stated |
Questionnaire survey |
Cross-sectional randomised |
Sanitation |
|
Fiasorgbor |
2013 |
Accra - Nima, Teshie |
Low-income urban neighbourhoods, Nima - migrant, Teshie - indigenous |
Not stated |
Interviews, Field Observations |
Mixed methods |
Sanitation |
|
Kwarteng et al., |
2015 |
Abuakwa |
120 individuals Low-income urban neighbourhoods |
2013-2014 |
Survey |
Cross-sectional quantitative survey |
Sanitation |
|
Kabange and Nkansah |
2015 |
Kumasi |
Peri-urban predominantly muslim. 133 respondents |
Not stated |
Interviews, Field Observations |
Experts' ranking analysis |
Sanitation |
|
Greenland et al., |
2016 |
Kumasi |
Female Household Head, poor neighbourhoods, 400 Households |
Not stated |
Survey/Questionnaire |
Cross-sectional survey, Focus group |
Safe sanitation, Handwashing practices |
|
Crocker et al., |
2017 |
Central, Upper West and Volta regions |
Household Head Rural |
2012-2014 |
Survey |
Cluster-randomised design |
Sanitation |
|
Hurd et al., |
2017 |
Accra |
Household |
2011-2012 |
Survey |
Survey and Structured Observation |
Sanitation |
|
Akpakli et al., |
2018 |
South-eastern |
Households 16,353, Rural |
2013 |
Survey |
Logistic Regression Analysis |
Sanitation |
|
Ritter et al., |
2018 |
Accra |
Low-income urban neighbourhoods |
2012 |
Survey |
Random cross-sectional sampling |
Sanitation |
4.2 Demographic differences in use of sanitation services
Only two studies were found which examined a relatively wide income demographic. In that by Akpakli et al., (2018) data was extracted from a wider extended population survey in comparison to the other identified studies which were conducted on a smaller scale in specific areas. The Akpakli et al., (2018) study found a distinct influence of income on access to sanitation services, with almost all respondents in the lowest-income quintile having no access to improved sanitation services. However, even the highest quintile income group still reported nearly a 70% use of unimproved sanitation services (Akpakli et al., 2018). Conversely, Mazeau et al., (2012) investigated three distinct neighbourhoods within one city where it was found that the highest-income area most frequently practised open defecation, due to the availability of open fields and a lack of public sanitation services. Within the relatively higher-income area of the Mazeau et al., (2012) study it was found only 9% of the households had private toilet facilities. In comparison, the lowest-income area had the greatest proliferation of private toilet facilities, at 24% of the study participants. The other studies which were identified were conducted in low-income areas - therefore there was generally little variation in the income of participants.
With the exception of the Akpakli et al., (2018) study, the majority of study participants reported a relatively low level of education, when education level was indicated. Monney et al., (2013) reported that only 2% of respondents had a tertiary education and 90% of respondents indicated that they were self-employed. Similar findings of low levels of higher education and predominantly self-employed/blue collar jobs were reported by the other studies.
Use of public and private sanitation services was found to be lowest among children. The reasons which were given for this varied: commonly cited reasons included a lack of financial ability to pay for sanitation services (Monney et al., 2013), safety fears predominantly focused on the potential for children to fall into latrine pits (Adubofour et al., 2012), and the long queues for use of the public services (Hurd et al., 2017). Children were therefore found to be the most likely demographic to defecate into either a disposal bag or a container (which was then emptied into a latrine or street sewer), or to practise open defecation. However, the presence of a private or shared compound (shared between a few families) latrine was found by Ritter et al., (2018) to be equated with a higher likelihood of latrine use by children.
Women were found to be more likely to avoid using either the public sanitation services or to practise open defecation - safety was commonly cited as the primary reason for this behaviour. Thus, after children, women were the most likely to defecate in containers or bags in the home environment. However, the attitude of women towards the use of public sanitation services was found to vary by area. In the study conducted by Fiasorgbor (2013) two areas within a city were studied. It was found that in the Nima neighbourhood, 95% of women reported that they would not use a public sanitation service due to their discomfort at queuing with men. Conversely, in the Teshie neighbourhood only 12% of women stated that they would not be comfortable using a public sanitation service (Fiasorgbor, 2013). The differences in these preferences is potentially explained by the difference in population: the Nima neighbourhood was predominantly comprised of migrant communities, whereas the Teshie neighbourhood is predominantly indigenous. Another instance that highlighted where female attitudes to defecation varied was reported by Hurd et al., (2017), who found that women working in the markets would practise a form of open defecation where they would defecate into containers at their market stalls so that they did not have to leave their location. The dislike of sharing sanitation services with the opposite gender was most commonly reported by women: in the study by Kabange and Nkansah (2015) 76 out of 82 women surveyed stated that they would prefer to not share public sanitation services with men.
The majority of studies did not examine in depth any differences due to religious practices. However, Kabange and Nkansah (2015) conducted a study in a lower-income neighbourhood that was predominantly Muslim. When questioned regarding their sanitation preferences it was found that Muslim preferred to face in a North-South position when defecating to prevent facing or turning their back on Mecca during the process. Similarly, it was reported that Muslim communities typically state a preference for flushing toilets over dry toilets due to the practice of using water for anal cleansing after defecating (Kabange and Nkansah, 2015).
If you need assistance with writing your dissertation, our professional Dissertation Writing Service is here to help!
Find out moreChapter 5 – Discussion
The findings of this study indicate that there is a low prevalence of private sanitation services in Ghana. Although the majority of studies were focused on low-income areas, some studies included research undertaken in relatively higher-income areas, and it was found that there was still a very low occurrence of private sanitation services. All studies indicated that there are public sanitation facilities available to the populations of the study areas. However, when examined in detail, all studies reported that at least a portion of the populations were hesitant to use these facilities. The reasons given for hesitance to use the public sanitation services varied; however, some reasons cited were common throughout all the studies. These commonly cited reasons included the relatively high cost of using the public sanitation services - this was particularly highlighted by respondents who were part of a large, low-income family. In one instance a female head of household responded that the cost of public sanitation use was a particular burden when members of the household were suffering from diarrheal diseases, and it was a financial burden that they were unable to afford (Hurd et al., 2017). The issue of cost was arguably the most cited reason for dislike of the public sanitation services available. Other reasons which were commonly given included the lack of management, smell, lack of privacy and the long queues for access. It is evident that the public sanitation services available in the low-income areas of Ghana are not suitable for purpose and improvements need to be made.
The poor quality of the public sanitation services in Ghana is likely the primary driving cause behind the continuation of open defecation and the practice of defecating in a bag or container at home before disposal with the household waste or in open street sewers. This is a significant cause for concern regarding the potential for fecal contamination of the home environment and the inappropriate disposal of fecal matter without treatment. It is likely that these practices increase the potential for disease transmission and contribute to the high incidence of diarrheal diseases in lower-income communities. Children under 5 years of age are known to be disproportionally impacted by diarrheal diseases. It was found during this study that young children are more likely to defecate in the home environment than use the public sanitation services. Safety concerns were frequently cited, with mothers afraid that their children would fall into the latrine pits commonly used in public sanitation services. Interestingly, it was also found that even when there were private latrines available, or shared compound latrines, young children were more unlikely to use these facilities than other family members due to similar safety fears (Adubofour et al., 2012), although Ritter et al., (2018) did highlight that there was a higher incidence rate of young children using latrines when they were private as opposed to public. This low rate of use of latrines or toilets by young children is a potential issue with regards to habit-forming and may potentially contribute to a reduced use of sanitation services as the children age.
An additional issue with children defecating in the home environment as opposed to the use of sanitation services is the potential for the spread of fecal matter which could contaminate the domestic environment. Curtis et al., (2000) reported that the contamination of the home environment, the child’s main habitat, with fecal matter can substantially increase the risk of diarrheal diseases. In situations such as those described in many of the identified studies, the safe disposal of fecal matter when children defecate in the home environment is not likely to be occurring. Many of the study respondents indicated that when defecating in the home environment, the fecal matter was disposed of in the household garbage. A secondary concern is the lack of handwashing facilities in the home environment of the majority of demographics covered in the identified studies. The mother is typically the primary caregiver in Ghanaian households and thus is the individual most likely to be disposing of the defecations of children. Studies have shown that when mothers do not wash their hands after coming into contact with fecal matter or defecation, there is an increased risk of their children contracting diarrheal diseases (Danquah et al., 2014). Thus, the frequent occurrence of children defecating in the home environment in low-income areas of Ghana is likely to be a significant contributing factor to the high prevalence of diarrheal disease among young children.
Whilst the majority of studies were focused on the prevalence of sanitation facilities and the defecation practices of the study participants, there were some limited cultural aspects to the use of sanitation services that were identified in the review. Not all of the studies characterised the religious beliefs of the study participants, but two studies did indicate that Muslim families in particular are likely to encounter religious cultural barriers to the use of sanitation services. One area of concern was the desire of Muslim individuals to not face Mecca or turn their back on Mecca when defecating as this is a sign of disrespect (Kabange and Nkansah, 2015). When questioned, many Muslim individuals stated that they prefer to face in a North-South orientation when defecating. This is a consideration which is unlikely to have been taken into account when designing and constructing sanitation services in low-income areas of Ghana. Therefore, the orientation of the sanitation services many present a concern and lead to Muslim individuals either choosing to defecation in an alternative manner or at alternative facilities. Additionally, the type of latrine/toilet facility which is provided is another area of concern as many Muslims use water for anal cleansing, primarily for religious reasons. Many of the latrines that are installed in public sanitation services are not conducive to the use of water for cleansing (Kabange and Nkansah, 2015). Ghana is a country which has a relatively high Muslim population, particularly in the Northern areas. The religious cultural preferences of the Muslim population constitute a factor which should be taken into account when developing sanitation services for public use.
The differences in sanitation services use between men and women is to some extent a cultural issue. This was exemplified in the study completed by Fiasorgbor (2013), which examined two communities, one predominantly comprised of migrants and one comprised of indigenous populations. One of the most obvious differences was seen in the attitudes of the female respondents to the use of public sanitation services, where 95% of the migrant females questioned did not use the public sanitation services as they did not like queuing with men to use the facilities. In comparison only 12% of the indigenous women reported similar feelings. As with the cultural Muslim behaviours, this example highlights how different cultural groups have different interpretations and perceptions of the use of sanitation services. However, given the choice, it is likely that the majority of the Ghanaian female population would prefer separate sanitation facilities, as other identified studies found that a lack of privacy and safety using the public sanitation services was an issue, particularly at night (Kwarteng et al., 2015). In some cultures, it is not acceptable for men and women to share the same sanitation services (Tanle and Kendie, 2013). Whilst it was not identified in any of the studies comprising this review, the lack of privacy aspect of sanitation services in Ghana has been identified as a particular issue for females experiencing menstruation in other studies (Kjellen et al., 2012; Sommer and Sahin, 2013).
It was found that attitudes towards open defecation varied. In some studies participants were found to have no issue discussing their participation in open defecation, whilst in other studies it was avoid due to an attached sense of shame. It is likely that these varying attitudes towards open defecation reflect cultural differences between different population groups. It can mean that it is difficult to accurately assess the true extent of open defecation in Ghana. What is evident from observation in addition to the testimonies of those who admit to practising open defecation is that this is still a significant issue in Ghana. The majority of participants who supplied a reason for open defecation was either that they were unable to afford to use sanitation services or that they actively preferred open defecation as the more comfortable option to the use of sanitation services which were smelly and unclean. In general, it was more commonly found that men or children would practise open defecation, and women were generally found to be more likely to defecate in the home environment if the sanitation services were unsuitable. It is therefore suggested that the issue of open defecation in Ghana is still a significant problem that can have substantial detrimental impacts on the health of the population and the spread of disease. Interestingly, in the studies which examined a variety of income populations, it was found that even those considered to have a relatively higher income were still found to practise open defecation.
Chapter 6 – Conclusions and Recommendations
6.1 Conclusions
In conclusion, it was found that sanitation services in Ghana are severely lacking among low-income populations. The lack of sanitation services is suggested to be accompanied by a lack of suitable hygiene practices, although there was insufficient focus on this aspect in the identified studies, with only a couple of studies commenting on handwashing practices as secondary observations. It was found that there is a very low prevalence of private sanitation services in the low-income areas of Ghana; additionally some studies considered areas of slightly higher income where it was still found that there was a very low prevalence of private sanitation services. The majority of individuals relied on the use of public sanitation services, defecated in the home environment bags or containers, or practised open defecation. The general perception of public sanitation services was that they were smelly, poorly managed, inconvenient and expensive, and lacked privacy.
There were found to be some indications of socio-cultural differences in the use of sanitation services. Women and children were found to be more likely to defecate in the home environment in bags or containers. For young children this was predominantly due to either a fear for their safety or the expense of public sanitation services. For women the reasons given varied, with the expense and dislike of queuing with men being the most commonly cited reasons. There was also found to be an influence of religion on the perception of sanitation services - Muslims in particular were found to have some religious restrictions on their sanitation practices, including the desire to not face Mecca when defecating and the need to use water for subsequent cleansing.
The relatively high rate of open defecation and the generally poor cleanliness standards of the public sanitation services available is a likely contributor to the high rates of diarrheal diseases in low-income populations. Young children in particular are more likely to be exposed to transmission of diseases due to the potential contamination of the home environment with fecal matter due to the twin reasons of at-home defecation and a lack of handwashing facilities for children and their mothers as primary caregivers.
It is evident that the current status of sanitation services in low-income areas of Ghana is unsatisfactory and are a highly likely contributor to the high rates of diarrheal diseases among these communities. There is an urgent need for action strategies to be implemented that can provide more appropriate solutions for sanitation services that take account of the cultural preferences of the population. If sanitation services are not improved, it is likely that the rate of diarrheal diseases and child mortality rates will not see significant decreases in the near future.
Overall the improvement of sanitation services in Ghana is likely to be a difficult and time-consuming undertaking which will require significant financial investment. However, it is a highly necessary undertaking to preserve the progress which has been made in the provision of safe water and to reduce the impact of disease and child mortality rates.
If you need assistance with writing your dissertation, our professional Dissertation Writing Service is here to help!
Find out more6.2 Recommendations
There is an urgent need for more appropriate sanitation services to be provided in the low-income areas of Ghana. From the findings of this study, it is evident that there are some socio-cultural factors which need to be taken into consideration when attempting to improve the provided sanitation services. The most commonly identified cultural factors influencing sanitation services were found to be religion and gender differences. Given the current lack of appropriate sanitation services, it is necessary that the different cultural preferences are taken into consideration when developing sanitation solutions, and it is recommended that research is undertaken into the demographic of an area before new sanitation services are provided.
The lack of desirable standards in sanitation services was a commonly cited reason for not using public sanitation services. It is thereby recommended that the standards of existing services need to be improved. A potential method of achieving this could be the establishment of an independent standards body responsible for the inspection of sanitation services.
In some low-income areas it is likely to be unfeasible for new sanitation services to be provided, often due to a lack of available space. In this instance it is likely that the practice of defecation in the home environment will continue. It is therefore recommended that research should be conducted regarding the potential provision of a safe disposal method of fecal matter produced in the home environment so that there is a reduction in the disposal of fecal matter in the municipal garbage system and street sewers. The appropriate treatment of waste matter is an issue of high concern when attempting to reduce the potential for the spread of disease and the contamination of water resources.
References
Acheampong, G.K. and Avorgbedor, Y.E., 2017. Determinants of under Five Mortality in Ghana; A Logistic Regression Analysis Using Evidence from the Demographic and Health Survey (1988-2014). American Journal of Public Health, 5(3), pp.70-78.
Adubofour, K., Obiri-Danso, K. and Quansah, C., 2013. Sanitation survey of two urban slum Muslim communities in the Kumasi metropolis, Ghana. Environment and Urbanization, 25(1), pp.189-207.
Akpakli, D.E., Manyeh, A.K., Akpakli, J.K., Kukula, V. and Gyapong, M., 2018. Determinants of access to improved sanitation facilities in rural districts of southern Ghana: evidence from Dodowa Health and Demographic Surveillance Site. BMC research notes, 11(1), p.473.
Akter, T. and Ali, A.M., 2014. Factors influencing knowledge and practice of hygiene in Water, Sanitation and Hygiene (WASH) programme areas of Bangladesh Rural Advancement Committee. Rural Remote Health, 14(3), p.2628.
Alagidede, P. and Alagidede, A.N., 2015. Meeting and missing targets: the public health dynamics of water and sanitation in Ghana. Journal of Public Health, 38(4), pp.e425-e429.
Arku, R.E., Bennett, J.E., Castro, M.C., Agyeman-Duah, K., Mintah, S.E., Ware, J.H., Nyarko, P., Spengler, J.D., Agyei-Mensah, S. and Ezzati, M., 2016. Geographical inequalities and social and environmental risk factors for under-five mortality in ghana in 2000 and 2010: Bayesian spatial analysis of census data. PLoS medicine, 13(6), p.e1002038.
Ashbolt, N.J., 2004. Microbial contamination of drinking water and disease outcomes in developing regions. Toxicology, 198(1-3), pp.229-238.
Assefa, M. and Kumie, A., 2014. Assessment of factors influencing hygiene behaviour among school children in Mereb-Leke District, Northern Ethiopia: a cross-sectional study. BMC public health, 14(1), p.1000.
Baker, K.K., O’Reilly, C.E., Levine, M.M., Kotloff, K.L., Nataro, J.P., Ayers, T.L., Farag, T.H., Nasrin, D., Blackwelder, W.C., Wu, Y. and Alonso, P.L., 2016. Sanitation and hygiene-specific risk factors for moderate-to-severe diarrhea in young children in the global enteric multicenter study, 2007–2011: case-control study. PLoS medicine, 13(5), p.e1002010.
Berendes, D., Kirby, A., Clennon, J.A., Raj, S., Yakubu, H., Leon, J., Robb, K., Kartikeyan, A., Hemavathy, P., Gunasekaran, A. and Ghale, B., 2017. The influence of household-and community-level sanitation and fecal sludge management on urban fecal contamination in households and drains and enteric infection in children. The American journal of tropical medicine and hygiene, 96(6), pp.1404-1414.
Centre for Science and Environment. 2018. Bottom to the fore: State of sanitation in Sub-Saharan Africa. Available online at: https://www.cseindia.org/bottom-to-the-fore-8624 (Accessed: 2/9/2018).
Cooper, H. (2003). Psychological Bulletin: Editorial. Psychological Bulletin, 129(1), 3-9.
Crocker, J., Saywell, D. and Bartram, J., 2017. Sustainability of community-led total sanitation outcomes: Evidence from Ethiopia and Ghana. International journal of hygiene and environmental health, 220(3), pp.551-557.
Curtis, V., Cairncross, S. and Yonli, R., 2000. Domestic hygiene and diarrhoea–pinpointing the problem. Tropical medicine & international health, 5(1), pp.22-32.
Danquah, L., Mensah, C.M., Agyemang, S. and Awuah, E., 2015. Risk factors associated with diarrhea morbidity among children younger than five years in the Atwima Nwabiagya District, Ghana: a cross-sectional study.
Dreibelbis, R., Jenkins, M., Chase, R.P., Torondel, B., Routray, P., Boisson, S., Clasen, T. and Freeman, M.C., 2015. Development of a multidimensional scale to assess attitudinal determinants of sanitation uptake and use. Environmental science & technology, 49(22), pp.13613-13621.
Eisenberg, J.N., Scott, J.C. and Porco, T., 2007. Integrating disease control strategies: balancing water sanitation and hygiene interventions to reduce diarrheal disease burden. American Journal of Public Health, 97(5), pp.846-852.
Feilzer, M.Y, 2010. Doing mixed methods research pragmatically: Implications for the rediscovery of pragmatism as a research paradigm. Journal of mixed methods research, 4(1), pp.6-16.
Fiasorgbor, D.A., 2013. Water and sanitation situation in Nima and Teshie, greater Accra Region of Ghana. Journal of Toxicology and Environmental Health Sciences, 5(2), pp.23-28.
Fuller, J.A., Westphal, J.A., Kenney, B. and Eisenberg, J.N., 2015. The joint effects of water and sanitation on diarrhoeal disease: a multicountry analysis of the Demographic and Health Surveys. Tropical Medicine & International Health, 20(3), pp.284-292.
Fuller, J.A., Goldstick, J., Bartram, J. and Eisenberg, J.N., 2016. Tracking progress towards global drinking water and sanitation targets: a within and among country analysis. Science of the Total Environment, 541, pp.857-864.
Greenland, K., de-Witt Huberts, J., Wright, R., Hawkes, L., Ekor, C. and Biran, A., 2016. A cross-sectional survey to assess household sanitation practices associated with uptake of “Clean Team” serviced home toilets in Kumasi, Ghana. Environment and urbanization, 28(2), pp.583-598.
Hetherington, E., Eggers, M., Wamoyi, J., Hatfield, J., Manyama, M., Kutz, S. and Bastien, S., 2017. Participatory science and innovation for improved sanitation and hygiene: process and outcome evaluation of project SHINE, a school-based intervention in Rural Tanzania. BMC public health, 17(1), p.172.
Hunter, P.R., 2003. Climate change and waterborne and vector‐borne disease. Journal of applied microbiology, 94, pp.37-46.
Hurd, J., Hennink, M., Robb, K., Null, C., Peprah, D., Wellington, N., Yakubu, H. and Moe, C.L., 2017. Behavioral influences on risk of exposure to fecal contamination in low-resource neighbourhoods in Accra, Ghana. Journal of Water Sanitation and Hygiene for Development, p.2017128.
JMP. 2017. Progress on Drinking Water, Sanitation and Hygiene 2017. Available online at: https://washdata.org/sites/default/files/documents/reports/2018-01/JMP-2017-report-final.pdf (Accessed: 15/9/2018).
Kabange, R.S. and Nkansah, A., 2015. Peri-urban community socio-cultural preferences for, and experts’ views on, sanitation options: a case study of the Kotoko community in Suame (Kumasi), Ghana. Journal of Environment and earth Science, 5(18), pp.28-35.
Khan, K.S., Kunz, R., Kleijnen, J. and Antes, G., 2003. Five steps to conducting a systematic review. Journal of the royal society of medicine, 96(3), pp.118-121.
Kjellén, M., Pensulo, C., Nordqvist, P. and Fogde, M., 2012. Global review of sanitation system trends and interactions with menstrual management practices. Report for the Menstrual Management and Sanitation Systems Project, Stockholm Environment Institute, Sweden, Project Report-2011.
Kumi-Kyereme, A. and Amo-Adjei, J., 2016. Household wealth, residential status and the incidence of diarrhoea among children under-five years in Ghana. Journal of epidemiology and global health, 6(3), pp.131-140.
Kwarteng, A.B., Williams Agyemang-Duah, F.A. and Agyemang, E., 2015. Assessing sanitation conditions and its impacts on the health status of urban dwellers in Abuakwa, Ghana. A Cross sectional survey. facilities, 5(17).
Lakshminarayanan, S. and Jayalakshmy, R., 2015. Diarrheal diseases among children in India: Current scenario and future perspectives. Journal of natural science, biology, and medicine, 6(1), p.24.
Lawrence, J.J., Yeboah-Antwi, K., Biemba, G., Ram, P.K., Osbert, N., Sabin, L.L. and Hamer, D.H., 2016. Beliefs, behaviors, and perceptions of community-led total sanitation and their relation to improved sanitation in rural Zambia. The American journal of tropical medicine and hygiene, 94(3), pp.553-562.
Liu, L., Oza, S., Hogan, D., Chu, Y., Perin, J., Zhu, J., Lawn, J.E., Cousens, S., Mathers, C. and Black, R.E., 2016. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. The Lancet, 388(10063), pp.3027-3035.
Mara, D., Lane, J., Scott, B. and Trouba, D., 2010. Sanitation and health. PLoS medicine, 7(11), p.e1000363.
Mazeau, A.P., Scott, R.E. and Tuffuor, B., 2012. Sanitation-a neglected essential service in the unregulated urban expansion of Ashaiman, Ghana. IN: Proceedings of Sustainable Futures Conference: Architecture and Urbanism in the Global South, Kampala, Uganda, 25-30 June 2012, pp. 37-44.
Monney, I., Buamah, R., Odai, S.N., Awuah, E. and Nyenje, P.M., 2013. Evaluating access to potable water and basic sanitation in Ghana’s largest urban slum community: Old Fadama, Accra. Journal of Environment and Earth Science, 3(11), pp.72-79.
Monney, I. and Antwi-Agyei, P., 2018. Beyond the MDG water target to universal water coverage in Ghana: the key transformative shifts required. Journal of Water Sanitation and Hygiene for Development, 8(2) p.127-141
Montgomery, M.A. and Elimelech, M., 2007. Water and sanitation in developing countries: including health in the equation. Available online at: http://www.unc.edu/courses/2007spring/envr/890/003/readings/010107feature_elimelech.pdf (Accessed: 14/9/2018).
Munamati, M., Nhapi, I. and Misi, S., 2016. Exploring the determinants of sanitation success in Sub-Saharan Africa. Water research, 103, pp.435-443.
NCWSS. 2014. National Community Water and Sanitation Strategy. Available online at: https://www.washghana.net/sites/default/files/National+Community+Water+and+Sanitation+Strategy+(NCWSS).pdf (Accessed: 15/9/2018).
Oloruntoba, E.O., Folarin, T.B. and Ayede, A.I., 2014. Hygiene and sanitation risk factors of diarrhoeal disease among under-five children in Ibadan, Nigeria. African health sciences, 14(4), pp.1001-1011.
O’reilly, K. and Louis, E., 2014. The toilet tripod: Understanding successful sanitation in rural India. Health & place, 29, pp.43-51.
Pfadenhauer, L.M. and Rehfuess, E., 2015. Towards effective and socio-culturally appropriate sanitation and hygiene interventions in the Philippines: a mixed method approach. International journal of environmental research and public health, 12(2), pp.1902-1927.
Prüss, A., Kay, D., Fewtrell, L. and Bartram, J., 2002. Estimating the burden of disease from water, sanitation, and hygiene at a global level. Environmental health perspectives, 110(5), p.537.
Prüss‐Ustün, A., Bartram, J., Clasen, T., Colford Jr, J.M., Cumming, O., Curtis, V., Bonjour, S., Dangour, A.D., De France, J., Fewtrell, L. and Freeman, M.C., 2014. Burden of disease from inadequate water, sanitation and hygiene in low‐and middle‐income settings: a retrospective analysis of data from 145 countries. Tropical Medicine & International Health, 19(8), pp.894-905.
Ritter, R.L., Peprah, D., Null, C., Moe, C.L., Armah, G., Ampofo, J., Wellington, N., Yakubu, H., Robb, K., Kirby, A.E. and Wang, Y., 2018. Within-Compound Versus Public Latrine Access and Child Feces Disposal Practices in Low-Income Neighbourhoods of Accra, Ghana.
Rheingans, R., Cumming, O., Anderson, J. and Showalter, J., 2012. Estimating inequities in sanitation-related disease burden and estimating the potential impacts of pro-poor targeting. London: SHARE: Sanitation and Hygiene Applied Research for Equity.
Rolfe, G., 2006. Validity, trustworthiness and rigour: quality and the idea of qualitative research. Journal of advanced nursing, 53(3), pp.304-310.
Sobh, R. and Perry, C., 2006. Research design and data analysis in realism research. European Journal of marketing, 40(11/12), pp.1194-1209.
Sommer, M. and Sahin, M., 2013. Overcoming the taboo: advancing the global agenda for menstrual hygiene management for schoolgirls. American journal of public health, 103(9), pp.1556-1559.
Tanle, A. and Kendie, S.B., 2013. Sanitation: A drawback to achieving the Millennium Development Goals? The situation in Ghana. Journal of Arts and Social Sciences, Faculty of Social Sciences, University of Cape Coast, 1(2):125-147, 2013
UN. 2016. Clean Water and Sanitation: Why it matters. Available online at: https://www.un.org/sustainabledevelopment/wp-content/uploads/2016/08/6_Why-it-Matters_Sanitation_2p.pdf (Accessed: 2/9/2018).
UN. 2018. Water and Sanitation. Available online at: http://gh.one.un.org/content/unct/ghana/en/home/our-work/sustainable-environment-energy-human-settlement/water-and-sanitation.html (15/9/2018).
UNESCO. 2017. The United Nations World Water Development Report 2017. Available online at: http://unesdoc.unesco.org/images/0024/002475/247552e.pdf (Accessed: 15/9/2018).
Wang, Y., Moe, C.L., Null, C., Raj, S.J., Baker, K.K., Robb, K.A., Yakubu, H., Ampofo, J.A., Wellington, N., Freeman, M.C. and Armah, G., 2017. Multipathway quantitative assessment of exposure to fecal contamination for young children in low-income urban environments in Accra, Ghana: the SaniPath analytical approach. The American journal of tropical medicine and hygiene, 97(4), pp.1009-1019.
Water. 2018. Ghana. Available online at: https://water.org/our-impact/ghana/ (Accessed: 15/9/2018).
WHI/UNICEF. 2017. ‘2017 Annual Report’. Available online at: https://washdata.org/sites/default/files/documents/reports/2018-07/JMP-2017-annual-report.pdf (Accessed: 15/9/2018).
WHO. 2018. Sanitation. Available online at: http://www.who.int/news-room/fact-sheets/detail/sanitation (Accessed: 2/9/2018).
Williams, D.R., Priest, N. and Anderson, N.B., 2016. Understanding associations among race, socioeconomic status, and health: Patterns and prospects. Health Psychology, 35(4), p.407.
Wolf, J., Prüss‐Ustün, A., Cumming, O., Bartram, J., Bonjour, S., Cairncross, S., Clasen, T., Colford Jr, J.M., Curtis, V., De France, J. and Fewtrell, L., 2014. Systematic review: assessing the impact of drinking water and sanitation on diarrhoeal disease in low‐and middle‐income settings: systematic review and meta‐regression. Tropical Medicine & International Health, 19(8), pp.928-942.
Wolf, J., Hunter, P.R., Freeman, M.C., Cumming, O., Clasen, T., Bartram, J., Higgins, J.P., Johnston, R., Medlicott, K., Boisson, S. and Prüss‐Ustün, A., 2018. Impact of drinking water, sanitation and handwashing with soap on childhood diarrhoeal disease: updated meta‐analysis and meta‐regression. Tropical medicine & international health, 23(5), pp.508-525.
Wright, J., Dzodzomenyo, M., Wardrop, N., Johnston, R., Hill, A., Aryeetey, G. and Adanu, R., 2016. Effects of sachet water consumption on exposure to microbe-contaminated drinking water: household survey evidence from Ghana. International journal of environmental research and public health, 13(3), p.303.
Cite This Work
To export a reference to this article please select a referencing style below: